Tennessee: Locals take back control to guarantee smokefree air for everyone.
No one in Tennessee is covered by a smokefree Workplace, Restaurant, and Bar law...yet!
Tennessee is home to more than 6 million residents. From the Smoky Mountains to the country music capital of the world, residents and visitors of the Volunteer state are not fully protected by strong smokefree laws. In 2007, a weak statewide smokefree law went into effect with exemptions including small workplaces with 4 or fewer employees as well as restaurants and bars prohibiting entry for those 21 and under. Both of these are tobacco industry-sponsored exemptions meant to limit smokefree protections. Millions of residents are left behind by a weak partial statewide law and remain exposed to secondhand smoke.
- 62.3% of Americans enjoy comprehensive smokefree protections in all public places and workplaces, including restaurants and bars. In contrast, in Tennessee 0% of the population is protected by this type of smokefree law. [2]
- Tennessee is 1 of 10 “Most Challenged” states based on health outcomes according to the United Health Foundation’s “America’s Health Rankings Annual Report,” ranking 41st out of 50 and 42nd in Non-smoking Regulations. [3]
- In a historic win, preemption was repealed in 2022 restoring local authority of smokefree protections in age-restricted venues.
- 41 college campus sites in the state are 100% smokefree, of which 37 are tobacco-free. [4]
- 125,000 Tennesseans currently under the age of 18 will die prematurely from smoking. [5]
- Healthcare costs attributed to tobacco use in Tennessee amount to $2.67 billion annually. [6]
Preemption Status:
Partially Preempted
May pass laws in 21+ venues
Preemption refers to situations in which a law passed by a higher level of government takes precedence over a law passed by a lower one. Preemption is a tobacco industry tactic that removes a community’s right to enact local smokefree air laws.
Since 1994, Tennessee state law has preempted local authority from adopting smokefree air and other tobacco control laws. Private businesses can adopt a policy making their business smokefree, but municipalities were not able to pass a city-wide law prohibiting smoking in workplaces, restaurants, and bars. Local control was partially restored in 2022; municipalities may now adopt smokefree laws in age-restricted (21+) venues such as bars and music clubs.


Musicians in Tennessee are Exposed to Secondhand Smoke
Current Landscape of Smokefree Protections
Preemption: Big tobacco's playbook
No one in Tennessee is currently protected by a 100% workplace, restaurant, and bar law. Thousands of employees, patrons, and visitors are exposed to secondhand smoke in these venues. The state Nonsmokers’ Protection Act has problematic exemptions for small businesses, and in restaurants and bars that prohibit patrons under 21 from entering. The exemptions affect some of the nation’s most beloved performers who remain exposed to secondhand smoke when touring and sharing their art in Tennessee. Nashville and Memphis are very high-profile tourist destinations known for live performances and a rich history with the music industry. In 2022, preemption of local municipalities to regulate smoking in age-restricted venues was lifted. Now cities in Tennessee have the option to address smoking in these businesses where musicians and hospitality workers remain exposed to secondhand smoke.
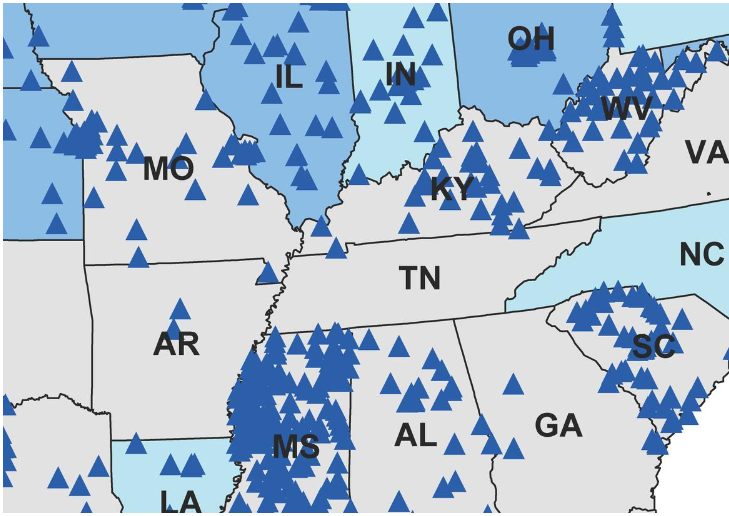
Tennessee: A Blank Slate for Smokefree Local Laws
Tennessee is a blank slate when it comes to smokefree laws. Because state law previously preempted local governments from implementing any kind of smokefree laws in Tennessee municipalities for the last two decades, it has fallen behind the rest of the nation in protecting its citizens from secondhand smoke. Reversing preemption and restoring local control is the clear solution to improve health, save lives, attract and retain the best talent to the Volunteer State. The triangles on the map represent municipalities with laws requiring 100% smokefree workplaces, restaurants, and bars. At the state level, blue represents a statewide law requiring 100% smokefree workplaces, restaurants, and bars and turquoise represents state laws requiring one or two of those components; grey represents no 100% smokefree provisions. Note that the map does not reflect American Indian sovereign tribal policies.
musicians take center stage on smokefree air
The music industry and the tourism dollars it generates are a primary source of revenue for the state of Tennessee. Yet musicians and hospitality workers remain among those most exposed to secondhand smoke.
Several artists lent their voices to the effort to repeal preemption and protect musicians in their workplace, sharing their personal stories about secondhand smoke exposure and joining Musicians for a Smokefree Tennessee. The collaborative efforts of artists, music venues and fans caught the attention of decision makers in a state where progress on smokefree air had come to a standstill.
These same artists, joined by local, state and national public health partners will play a crucial role in building support for local smokefree air policy change.


Who is left behind?
Tennessee lags behind the rest of the country when it comes to protecting nonsmokers from secondhand smoke in public places and workplaces. Allowing smoking in workplaces, restaurants, and bars is not only leaving thousands of people exposed to the hazardous chemicals in secondhand smoke, but it also normalizes the act of smoking in public. Outside of metro areas, rural Tennessee residents are also left vulnerable to secondhand smoke exposure.
Thousands of workers continue to be exposed to secondhand smoke in exempted venues including smoking areas of restaurants, bars, and private clubs. Those living in Tennessee rank their own and their children’s health status as worse than the rest of the country. [7] Various social determinants and behaviors continue to consistently land the state in the bottom 10 of health rankings lists. These are: economic disparity, lack of insurance, higher rates of smoking, and lower rates of physical activity, and they contribute to chronic conditions like heart disease, cancer, and stroke. There is a widening gap between rural and urban areas of the state, which is especially a concern, since 1.5 million people – 22% of the state’s population – reside in a rural area. Those living in a rural area face unique demographic, economic, and health access challenges. They are also more likely to be elderly, engage in unhealthy behaviors, and have lower incomes. [7] To overcome this disparity and ensure protection from secondhand smoke no matter your zip code, a broad-based coalition of support will be necessary.
Musicians are the heartbeat of Tennessee and Nashville, the state’s capitol, touts itself as America’s Music City. Musicians and performers as well fans and audiences across the state continue to be exposed to secondhand smoke in music venues.
Poor Health Outcomes and High Costs
Tobacco use is the leading preventable cause of death in the United States. More than 480,000 people die from smoking or exposure to secondhand smoke each year. [5]
Tennessee’s smoking rate among adults is 19.5% and 7.1% for high school students, compared to national rates of 14% and 8%, respectively. Tobacco exacts a high toll, with 11,400 Tennessee residents dying each year of tobacco-related illness. [6] At current trends, 125,000 kids under the age of 18 in Tennessee are projected to die prematurely from tobacco-related illness. [5]
Annual health care costs in the state directly caused by tobacco use are $2.67 billion ($823.6 million of which is Medicaid expenditures). [6]
Secondhand smoke exposure causes heart disease, stroke, and lung cancer among adults, as well as respiratory disease, ear infections, sudden infant death syndrome, more severe and frequent asthma attacks, and slowed lung growth in children. [5,8]
Beyond secondhand smoke exposure, nonsmokers exposed to thirdhand smoke in a casino are at an ever higher risk than those in a thirdhand smoke-polluted home. [9] Further, hospitality workers and children are susceptible to thirdhand smoke exposure, as the particles cling to hair, clothing and cars. Young children are particularly vulnerable, because they can ingest tobacco residue by putting their hands in their mouths after touching contaminated surfaces. [10]
Smokefree laws help to reduce adult smoking prevalence and prevent youth and young adult smoking initiation. [5,8]

COVID Reminds Us That Health Promotion Policies Matter
Smoking and vaping, along with exposure to secondhand smoke and aerosols, negatively impact the respiratory system and may cause a person’s immune system to not function properly, known as being immunocompromised. Research demonstrates that current and former smokers of any age are at higher risk of severe illness from coronavirus disease (COVID) in part due to compromised immune and/or respiratory systems. Smoking leads to cardiovascular disease, as well as respiratory illnesses including bronchitis, asthma, Chronic Obstructive Pulmonary Disease (COPD), and lung cancer as a result of exposure to particulate matter, toxins, and carcinogens into their lungs. Secondhand tobacco and marijuana smoke and aerosol contain many of the same toxins, carcinogens, and particulate matter that lead to respiratory and cardiovascular diseases.
Removing masks to smoke or vape indoors undermines the proven benefit of face coverings and increases the risk of transmitting or inhaling COVID via infectious respiratory droplets, uncovered coughs, and increased touching of faces. Preventing exposure to secondhand smoke and e-cigarette aerosol or vape by adopting a smokefree policy with no smoking or vaping indoors and moving smoking or vaping to socially distanced outdoor areas away from entrances, could help mitigate worker and public exposure to carcinogens and toxins, as well as COVID.
Just as social distancing and handwashing help prevent the spread of disease, eliminating secondhand smoke is critical to prevent acute and chronic diseases, and saves lives by reducing the risk of heart disease, stroke, respiratory diseases, and lung cancer by up to 30% at a population wide level.
Going smokefree prevents exposure to the carcinogens and toxins in secondhand tobacco and marijuana smoke as well as dramatically reduces the spread of respiratory droplets that could transmit flu and other viruses like COVID.
Strategies to Close Gaps & Increase Health Equity

Focus on smokefree policies: Competing issues can distract and delay work on smokefree policies. Smokefree laws have immediate and long-term health and economic benefits: they are worth the investment of time and effort to protect everyone from exposure to a known human carcinogen. [5]

Let local lead the way: Now that preemption has been repealed, there is an opportunity to let local lead the way. Advocates in cities like Nashville and Memphis are on the ready to build strong coalitions and pass smokefree air ordinances. Success at the local level demonstrates demand for smokefree air and will recruit additional champions for smokefree air to move towards further movement at the statewide level.
Adopt a statewide smokefree law: Since communities in Tennessee were preempted from adopting strong local smokefree laws for so long, thousands of employees remain exposed to secondhand smoke at work. Efforts focused on the legislature to adopt a comprehensive 100% smokefree workplace law that includes restaurants, bars, and casinos would be time well spent to close gaps in protections.
Statewide campaigns are always a challenge given the influence of the tobacco industry in state legislatures, particularly in southern states like Tennessee. Due to a lack of investment in building a local infrastructure to support smokefree policy change, grassroots and policy champions need to be recruited to move forward. Legislators need to hear from constituents that there is demand for smokefree workplace protections for all at the local and the statewide level.

Increase funding and resources: Tobacco prevention, education, training and cessation funds are needed to better address disparities in smoking and exposure to secondhand smoke. In addition, funds to support the implementation of a statewide law are critical to increase community awareness of and compliance with the smokefree rules.

Invest in the future: In order to address the gaps in smokefree coverage, a great deal of effort and financial resources will be required to explain the ongoing disparities in smokefree protections and the benefits of 100% smokefree environments, and to counter misinformation about the viability of ventilation systems to protect people from secondhand smoke exposure. Collaborating with and mobilizing additional community-based partners who represent those individuals or specific classes of workers being left behind is critical to reach success.
Sources of data:
- U.S. Environmental Protection Agency, Respiratory Health Effects of Passive Smoking: Lung Cancer and Other Disorders,” EPA/600/6-90/006F, December 1992.
- American Nonsmokers’ Rights Foundation. U.S. Tobacco Control Laws Database. Berkeley, CA, 2021.
- United Health Foundation. (2018). America’s Health Rankings Annual Report.
- American Nonsmokers’ Rights Foundation. U.S. College Campus Tobacco Policies Database. Berkeley, CA, 2018.
- US Department of Health and Human Services. The health consequences of smoking: 50 years of progress. A report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, CDC; 2014.
- Centers for Disease Control and Prevention. (n.d.). State Highlights: Tennessee [from State Tobacco Activities Tracking and Evaluation System].
- The Sycamore Institute. Healthy Debate 2018: Health and Well Being in Tennessee.
- US Department of Health and Human Services. Preventing tobacco use among youth and young adults. A report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, CDC; 2012.
- Matt, Dr. Georg (2018). Smoking Bans May Not Rid Casinos of Smoke. US News and World Report.
- Matt, G E, Quintana PJ E, Hovell MF et. al. (2004). Households contaminated by environmental tobacco smoke: sources of infant exposures. British Medical Journal: Tobacco Control.
- Grana, R; Benowitz, N; Glantz, S. “Background Paper on E-cigarettes,” Center for Tobacco Control Research and Education, University of California, San Francisco and WHO Collaborating Center on Tobacco Control. December 2013.
- Williams, M.; Villarreal, A.; Bozhilov, K.; Lin, S.; Talbot, P., “Metal and silicate particles including nanoparticles are present in electronic cigarette cartomizer fluid and aerosol,” PLoS ONE 8(3): e57987, March 20, 2013.
Related Reading:
Huang, J., King, B.A., Babb, S.D., Xu, X., Hallett, C., Hopkins, M. (2015). Socio-demographic disparities in local smokefree law coverage in 10 states. American Journal of Public Health, 105(9), 1806–1813.
Tynan, M.A., Baker Holmes, C., Promoff, G., Hallett, C., Hopkins, M., & Frick, B. (2016). State and local comprehensive smoke-free laws for worksites, restaurants, and bars — United States, 2015. Morbidity and Mortality Weekly Report, 65(24), 623-626.
[n.a.], “Tobacco industry interference with tobacco control,” Geneva: World Health Organization (WHO), 2008.
NCI Monograph 17: Evaluating ASSIST – A Blueprint for Understanding State-level Tobacco Control Evaluation of American Stop Smoking Intervention Study for Cancer Prevention Chapter 8, Evaluating Tobacco Industry Tactics as a Counterforce to ASSIST (October 2006).
July 2022